Immunohistochemistry (IHC) is a technique that involves the labeling of cellular proteins in tissue samples with a specific primary antibody and visualization of the target with detection reagents. Using IHC, protein expression can be assessed via chromogenic or fluorescent detection. Both detection systems rely on antigen recognition mediated by a primary antibody. Chromogenic IHC utilizes enzyme-catalyzed deposition of chromogens at the site of the antigen, while fluorescent IHC employs fluorophores and direct or indirect immunofluorescence to help visualize antigens of interest.
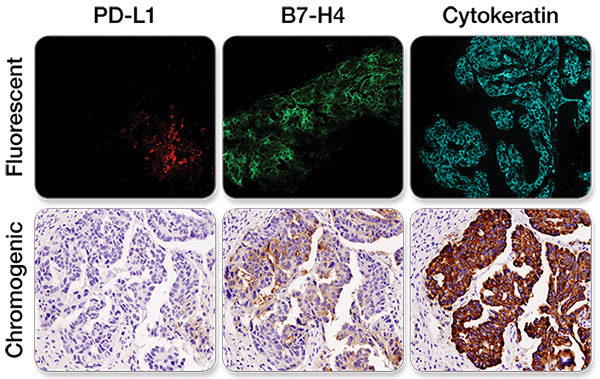
Immunohistochemical staining was performed on serial sections of ovarian carcinoma using PD-L1 (E1L3N®) XP® Rabbit mAb #13684 (left), B7-H4 (D1M8I) XP® Rabbit mAb #14572 (middle), and Pan Keratin (C11) Mouse mAb #4545 to evaluate the pattern and level of expression of these two immune checkpoint proteins using fluorescent and chromogenic detection systems. Note: the images taken were of different fields of view.
Both detection systems reveal equivalent detail of protein level and distribution. Thus, the choice of a detection method is entirely dependent on the objective of the experiment.
IHC is commonly used for morphological characterization of tumors or other tissue malignancies. IHC uses antibodies to detect and analyze protein expression while maintaining the composition, cellular characteristics, and structure of the native tissue.
At CST, scientists specializing in IHC test a large number of antibodies and only recommend those best suited for IHC - ensuring your assay will work the first time, every time.
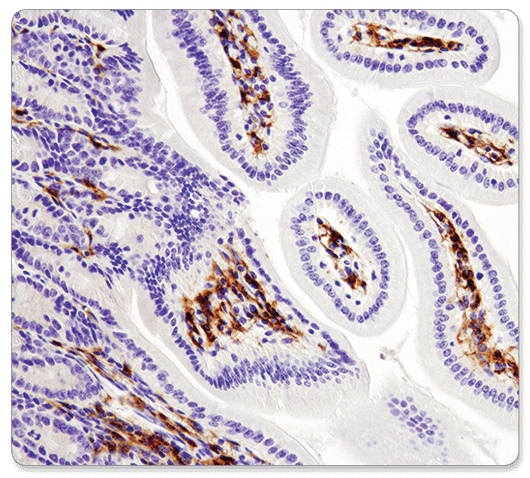
F4/80 (D2S9R) XP® Rabbit mAb #70076: IHC analysis of paraffin-embedded mouse small intestine using #70076.
At CST, scientists specializing in IHC test a large number of antibodies and only recommend those best suited for the application. Our scientists test multiple methods of antigen retrieval and immunostaining to determine the optimal conditions for use of each antibody in IHC. In addition, our scientists develop companion reagents for IHC to enhance antigen detection and improve the efficiency of IHC protocols.
The crosslinks created during the fixation step can prevent antibody binding by inhibiting access to the antigen; therefore, it is important to reverse crosslinks using a procedure called antigen retrieval. Antigen retrieval can be achieved through either a heat-induced method or enzymatic digestions. The recommended method for your CST antibody will be clearly indicated on the product datasheet.
The primary antibody is a critical component of any IHC assay and has a direct effect upon data quality. A poor primary antibody can result in uninterpretable or misleading results. It takes more than just positive staining in a single tissue sample for an antibody to be approved for use in IHC. Antibodies should undergo a stringent validation procedure to ensure that the antibody detects the target accurately.
Using the optimal reagents and protocols for your antibody can greatly improve your results.
You must also ensure the signal you are detecting is specific. An important consideration in any experiment is the inclusion of appropriate controls. Positive and negative controls instill confidence that your antibody is detecting its intended target.
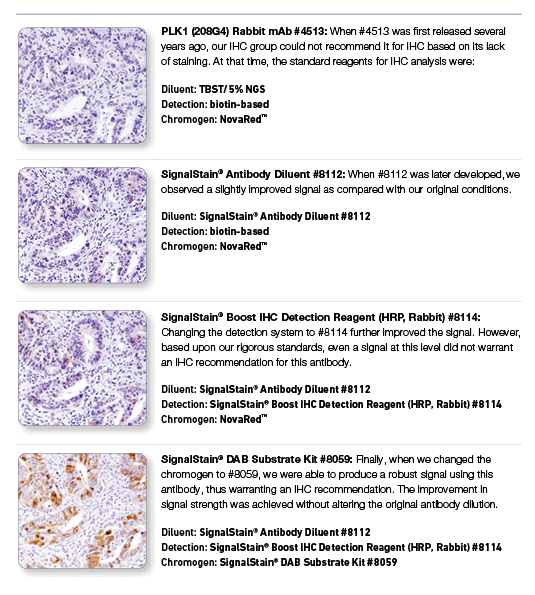
PLK1 (208G4) Rabbit mAb #4513: IHC analysis of paraffin-embedded human colon carcinoma using #4513 with step-by-step reagent substitution, as indicated, demonstrating that reagents can make the difference between poor staining and publishable results.
Suboptimal IHC staining is frequently resolved by adjusting relatively few variables. Adjustments to key steps within the protocol, such as antigen retrieval, can often resolve common issues, such as little or no signal and high background.
Contact our advanced technical support team to answer questions about your assay, including detailed information on:
The primary antibody is a critical component of any IHC assay and has a direct effect on data quality. The determination of target specificity in IHC analysis requires multiple validation steps. CST offers over 700 recombinant monoclonal antibodies that have been rigorously validated for IHC using formalin-fixed, paraffin-embedded (FFPE) tissues. In-house validation allows our scientists to provide expert advice that will save you time and accelerate your results. Our extensive validation ensures that all of our IHC-P validated antibodies can also be used for fluorescent multiplex IHC.
CST scientists use a variety of methods, as appropriate, to validate each IHC-recommended antibody, ensuring that the staining you observe with each antibody is specific. Validation steps include:
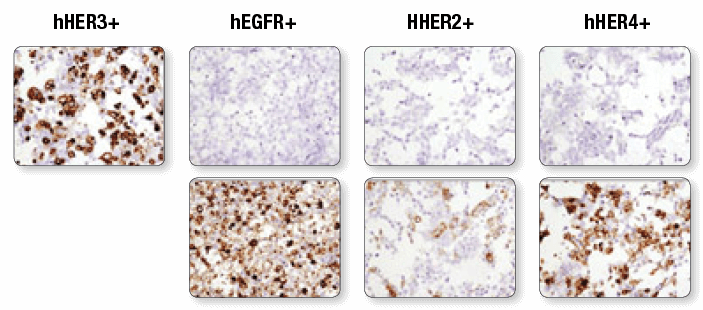
Immunohistochemical analysis of paraffin-embedded 293T cell pellets transfected with human erbB family members HER3, EGFR, HER2 and HER4 (from left to right as indicated) using HER3/ErbB3 (D22C5) XP® Rabbit mAb #12708 (top panels). Transfections were confirmed using EGF Receptor (D38B1) XP® Rabbit mAb #4267 (lower left), HER2/ErbB2 (D8F12) XP® Rabbit mAb #4290 (lower middle) and HER4/ErbB4 (111B2) Rabbit mAb #4795 (lower right).
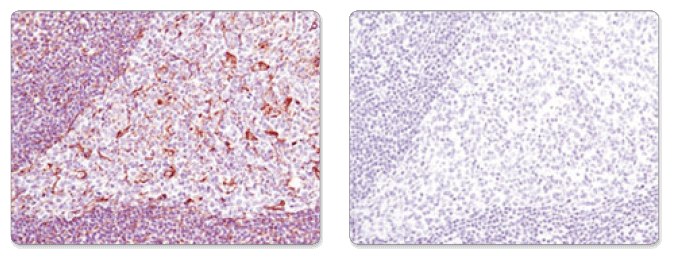
Immunohistochemical analysis of paraffin-embedded human tonsil using Vimentin (D21H3) XP® Rabbit mAb #5741 in the presence of control peptide (left) or antigen-specific peptide (right).
Immunohistochemistry IHC 3287 HCC78 xenograft
Antibodies are only one of the factors responsible for experimental success. Using the optimal reagents and protocols for your antibody can greatly improve your results. To improve the efficiency of your IHC protocol development and ensure your assay is successful, our scientists test multiple methods of antigen retrieval and immunostaining to determine the optimal conditions for use of each antibody in IHC. We develop companion reagents to enhance antigen detection, improving your results.
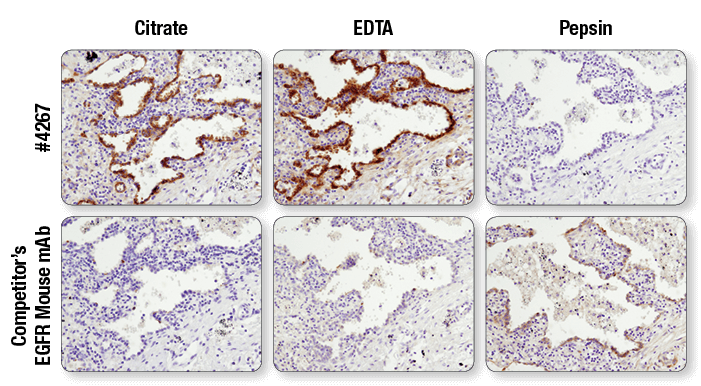
Antibodies targeting the same protein may have different preferred methods of antigen retrieval. IHC analysis of paraffin-embedded human lung carcinoma using EGF Receptor (D38B1) XP® Rabbit mAb #4267 and an EGFR mouse mAb after antigen retrieval by boiling in citrate buffer (left), boiling in EDTA buffer (center), or digestion with pepsin (right). For #4267, superior signal is obtained with EDTA retrieval. However, for the competitor’s EGFR mouse mAb, signal is only achieved with pepsin digestion.